
With COVID-19 cases surging, Nepal asks global community for urgent vaccine help

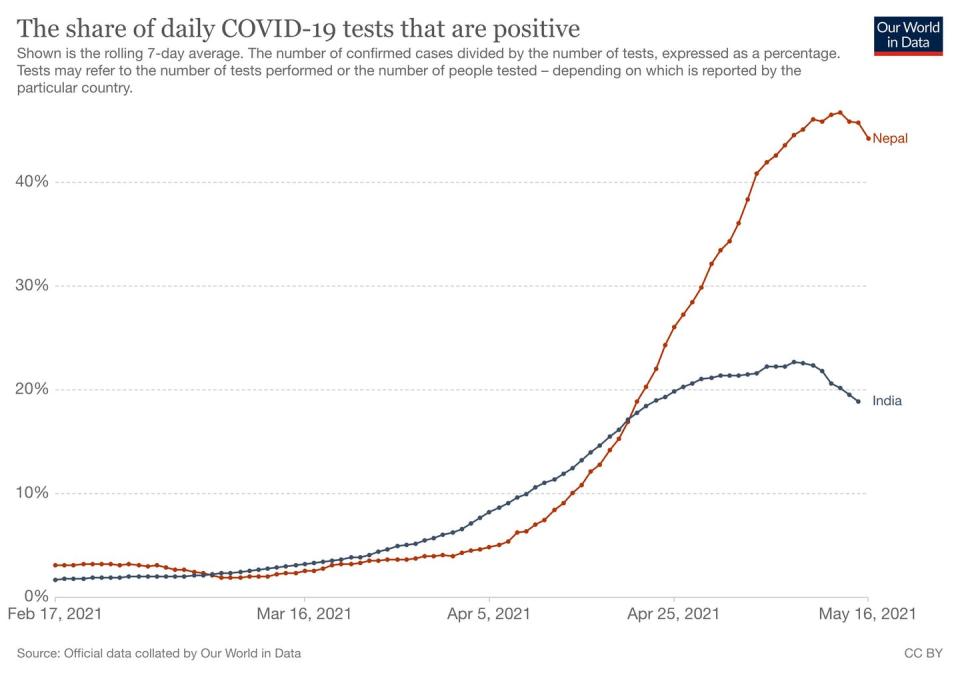
Nepal, the landlocked Himalayan country, currently has one of the highest COVID-19 viral reproduction rates in the world. The situation is dire: reports indicate Nepal has a consistently higher number of COVID-19 cases per million than India. By mid-July, new case numbers could reach 800,000, among a population of 30 million, with a predicted death toll of 40,000.
Last month, Nepal’s Ministry of Health said: “Since coronavirus cases have spiked beyond the capacity of the health system and hospitals have run out of beds, the situation is unmanageable.” The ministry also said it had no more vaccines.
Only two per cent of Nepal’s population is fully vaccinated. Nearly two million Nepalis have received their first dose of the AstraZeneca vaccine. However, with the halt of exports of vaccines from India, most have not had access to a second dose. This shortage of vaccines in Nepal has global epidemiological implications, such as the possibility of virus mutations that could readily spread regionally and beyond.
As social scientists and public health practitioners familiar with Nepal’s health-care delivery and emergency response systems, we recognize that ultimately, the capacity to care for people suffering from COVID-19 in Nepal is severely limited, with roughly 1,500 intensive care beds and just over 800 ventilators in the country. The mountainous terrain throughout much of the country, along with a lack of infrastructure, political marginalization and poverty compound the impacts of infectious disease.
However, we are also familiar with Nepal’s unique grassroots public health capacities, including the ability to quickly and effectively distribute vaccines to its people. Distributing vaccines to Nepal should help mitigate the country’s exigent crisis and help to flatten the curve in South Asia.
Inequalities mount
As North America and Europe return to semblances of normal life, the danger of creating and maintaining a “vaccine apartheid” is very real.
Vaccine apartheid refers to the idea that wealthy nations or groups get vaccines, while others do not. As World Health Organization Director General Tedros Adhanom Ghebreyesus says: “The solution is more sharing.”
Last week, in a positive step towards moving the needle on vaccine apartheid, U.S. President Joe Biden pledged an additional 20 million vaccine doses to share with the rest of the world. This is welcome news. However, Nepal has not been identified as a priority.
In 1816, during the global smallpox pandemic, Nepal’s King, Girvan Yuddha Bikram Shah, succumbed to the disease. Although at the time, Nepal, with assistance from India and Great Britain, was at the cutting-edge of global vaccine efforts, access to vaccines to protect its citizens remained elusive.
Today, as then, structural inequalities are exacerbated by the pandemic. Today, as then, Nepal is at the mercy of powerful global actors and faces a desperate humanitarian catastrophe.

As in India, Nepal has experienced a shortage of oxygen supplies for those who fall severely ill. The tolls of the virus roll down steep slopes of inequality impacted by social-structural factors like ethnicity, class, caste, geography and gender that co-mingle with public health policies. Nepal acutely illustrates how these differences exacerbated by a pandemic can lead to synergistic epidemics, or “syndemics.”
While aid in the form of cash, oxygen supply chain assistance and essential supplies for healthcare facilities are helpful, access to vaccines is paramount to stopping sickness and death.
Systems ready to distribute vaccines
Nepal is uniquely suited for vaccine aid. The country has demonstrated the successful implementation of a multi-sectoral COVID-19 vaccination program, in even some of its most remote regions.
If the Biden administration and its allies prioritize Nepal for emergency COVID-19 vaccines, there is evidence that Nepal could deliver them efficiently and effectively. The country has a track record of national vaccination initiatives and a grassroots public health infrastructure capable of reaching its population, not only for infectious disease but also for preventative care and the management of noncommunicable disease.
This infrastructure is neither confined to cities nor dependent on complex technologies; rather, it is anchored by people and rooted in places, cultures and languages in ways that can alleviate vaccine hesitancy and spread accurate public health knowledge.

For example, Nepal’s renowned 50,000-plus strong network of Female Community Health Volunteers is ready to travel the breadth of the country’s seven provinces, helping to reach every household in both urban and remote settings.
With coolers of AstraZeneca doses slung over their shoulders, well-worn sneakers and a will to serve their communities, Female Community Health Volunteers have delivered what vaccine supplies they had to the elderly and vulnerable.
Female Community Health Volunteers have been at the forefront of recent successful vaccine campaigns, achieving high rates of BCG, DPT, oral polio vaccine, measles-rubella and vitamin A supplementation coverage.
Physical distancing recommendations, isolation and sweeping lockdown measures are inapplicable in countries like Nepal, where many people live in close proximity and must leave the house for work and food.
Mobilizing, and supporting, Nepal’s community health workers to deliver vaccines, prioritizing the most heavily affected areas and moving out from there, demonstrates the need for localized approaches to pandemic control.
The extraordinary network of Female Community Health Volunteers is one example of the unique capacity in Nepal to deploy a well co-ordinated, robust, decentralized health-care system in service of its citizens. This type of nuanced, culturally appropriate, data-driven approach is needed if public health measures are to benefit the most vulnerable.
The crisis unfolding in Nepal and South Asia presents an imperative to the global community to deliver vaccine aid. It is also a call to recognize the work of grassroots, public health infrastructures in places like Nepal. This recognition can be critical to ending global health apartheid.
This article is republished from The Conversation, a nonprofit news site dedicated to sharing ideas from academic experts. It was written by: Katharine Rankin, University of Toronto; David Citrin, University of Washington; Galen Murton, James Madison University , and Sienna Craig, Dartmouth College.
Read more:
The authors do not work for, consult, own shares in or receive funding from any company or organisation that would benefit from this article, and have disclosed no relevant affiliations beyond their academic appointment.

